We investigated the longitudinal association of herpes zoster (HZ), commonly known as “shingles,” and long‐term risk of stroke or coronary heart disease (CHD) among participants in 3 large US cohorts, the NHS (Nurses' Health Study), NHS II (Nurses' Health Study II), and HPFS (Health Professionals Follow‐Up Study).
Methods and Results
Participants were 79 658 women in the NHS (2000–2016), 93 932 women in the NHS II (2001–2017), and 31 440 men in the HPFS (2004–2016), without prior stroke or CHD. Information on HZ, stroke, and CHD was collected on biennial questionnaires and confirmed by medical record review. Cox proportional hazards regression models were used to estimate multivariable‐adjusted hazard ratios for stroke and for CHD according to years since HZ compared with never HZ. During >2 million person‐years of follow‐up, 3603 incident stroke and 8620 incident CHD cases were documented. History of HZ was significantly and independently associated with higher long‐term risk of stroke and CHD. In pooled analyses, compared with individuals with no history of HZ, the multivariable‐adjusted hazard ratios (95% CIs) for stroke were 1.05 (0.88–1.25) among those with 1 to 4 years since HZ, 1.38 (1.10–1.74) for among those with 5 to 8 years since HZ, 1.28 (1.03–1.59) among those with for 9 to 12 years since HZ, and 1.19 (0.90–1.56) among those with ≥13 years since HZ. For CHD, the corresponding multivariable‐adjusted hazard ratios (95% CIs) were 1.13 (1.01–1.27) for 1 to 4 years, 1.16 (1.02–1.32) for 5 to 8 years, 1.25 (1.07–1.46) for 9 to 12 years, and 1.00 (0.83–1.21) for ≥13 years.
Conclusions
HZ is associated with higher long‐term risk of a major cardiovascular event. These findings suggest there are long‐term implications of HZ and underscore the importance of prevention.
From the
Channing Division of Network Medicine, Department of MedicineBrigham and Women’s Hospital BostonMA(S.G.C., E.B.R., G.C.C.);
Harvard Medical School BostonMA(S.G.C., K.K., K.M.R., E.B.R., G.C.C.);
Institutional Centers for Clinical and Translational ResearchBoston Children’s Hospital BostonMA(K.K.);
Department of ResearchOlmsted Medical Center RochesterMA(B.Y.);
Division of Women’s HealthBrigham and Women’s Hospital BostonMA(K.M.R.);
Department of NutritionHarvard T.H. Chan School of Public Health BostonMA(E.B.R.);
Department of EpidemiologyHarvard T.H. Chan School of Public Health BostonMA(E.B.R., G.C.C.);
Renal Division, Department of MedicineBrigham and Women’s Hospital BostonMA(G.C.C.).
Correspondence to: Sharon G. Curhan, MD, ScM, Channing Division of Network Medicine, Brigham and Women's Hospital, 181 Longwood Ave, Boston, MA 02115. Email:
scurhan@bwh.harvard.edu
This study demonstrates that herpes zoster is associated with an almost 30% higher long‐term risk of a major cardiovascular event.
●
The elevated risk of a major cardiovascular event may persist for ≥12 years following herpes zoster.
●
The elevated risk may be greater among those with potentially immunocompromising conditions or immunosuppressive treatments.
What Are the Clinical Implications?
●
These findings suggest there are long‐term cardiovascular implications of herpes zoster.
●
The availability of a safe and effective vaccine provides an opportunity to reduce the burden of herpes zoster and reduce the risk of subsequent cardiovascular complications.
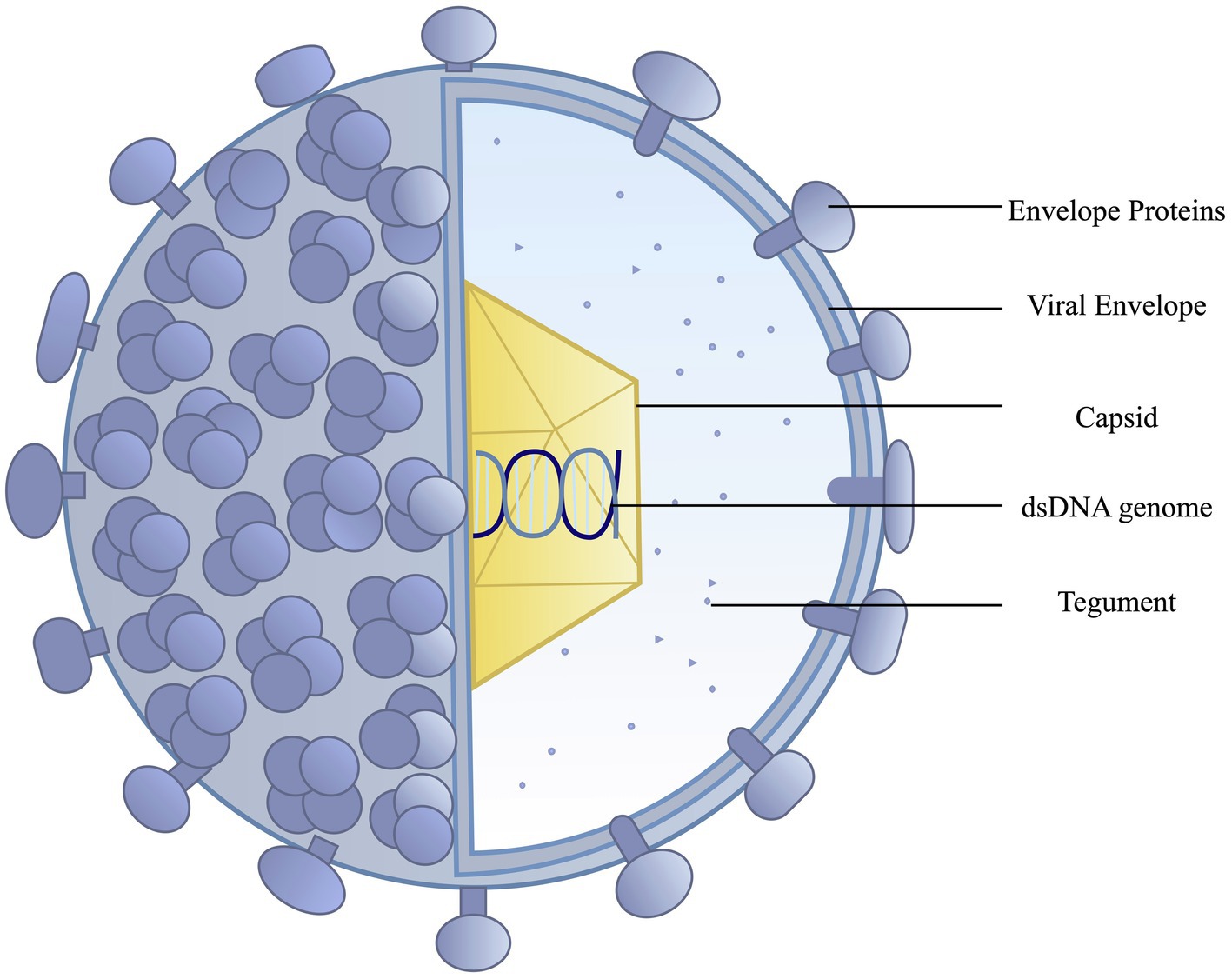
Almost all individuals aged ≥50 years in the United States have been infected with the varicella zoster virus (VZV) and therefore are at risk for the development of herpes zoster (HZ), or “shingles.” HZ occurs in both immunocompetent and immunocompromised individuals, and the incidence increases with age, reduced cell‐mediated immunity, or immunosuppressive therapy.
1,2,3,4Approximately 1 in 3 individuals will develop HZ during their lifetime, and the projected burden is expected to increase because of the demographic shift to a more aged population, increasing numbers of immunocompromised individuals, and increasing use of corticosteroids and immunosuppressive medications.
5,6,7,8,9
Several serious chronic complications of HZ can occur, most commonly postherpetic neuralgia
5and HZ ophthalmicus,
10but long‐term longitudinal information on HZ and risk of other adverse health outcomes is scant. VZV vasculopathy can complicate HZ and is caused by productive viral infection of the vasculature.
11A growing body of evidence suggests VZV‐related vasculopathy plays a role in the pathogenesis of cardiovascular disorders, including stroke and coronary heart disease (CHD).
11,12,13,14,15,16,17VZV has been detected in large and small blood vessels; and local inflammation, pathologic vascular remodeling, and chronic arterial changes can increase risk of subsequent vessel occlusion, ischemia, and a cardiovascular event.
18,19HZ‐related systemic inflammation, autoimmune responses, or hemodynamic changes could also lead to a cardiovascular event.
12,20,21Epidemiologic studies of HZ and risk of stroke and myocardial infarction (MI) demonstrate an increased risk of stroke and MI close to the HZ event
13; however, there is limited information on the long‐term association between HZ and cardiovascular events, particularly in the US population. Therefore, we prospectively investigated whether HZ is independently associated with higher long‐term risk of subsequent stroke or CHD in >200 000 women and men in 3 large ongoing US cohorts with long‐term follow‐up, the NHS (Nurses' Health Study), the NHS II (Nurses' Health Study II), and the HPFS (Health Professionals Follow‐Up Study). We also evaluated whether the associations differed among adults with potentially immunocompromising conditions.
Methods
The data that support the findings of this study are available from the corresponding author on reasonable request.
Study Population
The NHS was established in 1976 when 121 700 female registered nurses, aged 30 to 55 years, were enrolled by completing a baseline questionnaire. In 1989, the NHS II was established and enrolled 116 429 female registered nurses, aged 25 to 42 years. The HPFS began in 1986 and enrolled 51 529 male health professionals, aged 40 to 75 years. Participants completed questionnaires at baseline and every 2 years on a wide range of demographic, health, diet, and lifestyle factors, including detailed information on health history and medication use. The follow‐up rates in all 3 cohorts exceed 90% of eligible person‐time.
22,23For the present analyses, baseline was defined in each cohort based on the year when information on date of HZ event was first available through most recent follow‐up cycle (NHS: 2000–2016; NHS II: 2001–2017; and HPFS: 2004–2016). We excluded participants for whom the year of their HZ event was not provided and those with a history of stroke or CHD before study baseline. In total, 79 658 women in the NHS, 93 932 women in the NHS II, and 31 440 men in the HPFS were included in the analyses (total n=205 030). The Institutional Review Boards of Brigham and Women's Hospital and Harvard T.H. Chan School of Public Health approved the study protocol. The return of the questionnaires was considered to imply informed consent.
Ascertainment of HZ (“Shingles”)
Information on history of “shingles” (HZ) and the date it occurred was collected on the 2000, 2004, 2008, and 2012 NHS questionnaires, the 2001, 2005, 2013, and 2017 NHS II questionnaires, and the 2004, 2006, and 2008 HPFS questionnaires. Participants were asked about clinician‐diagnosed “shingles” and the year of diagnosis. To confirm the validity of self‐report in our participants, we mailed a supplemental questionnaire to 99 NHS women that asked for permission to obtain medical records relating to the diagnosis of shingles, which were reviewed by a physician investigator (G.C.C.). The diagnosis of HZ was confirmed in 97%, demonstrating that self‐reported diagnosis of shingles (HZ) in this cohort of nurses is highly reliable. Notably, the participants in all 3 of our cohorts are health care professionals, and the reliability of health‐related information collected from our participants has been demonstrated for a large number of health outcomes.
22The primary exposure for this study was categorized according to time (in years) since the participant's HZ event. Those with no history of HZ were the referent group.
Ascertainment of Stroke
Stroke was classified as total stroke, encompassing ischemic stroke and hemorrhagic stroke, confirmed by physician review of medical records according to criteria specified in the National Survey of Stroke,
24requiring evidence of a sudden or rapid onset of neurologic deficit that persisted for >24 hours or until death. Participants who reported a nonfatal stroke on a biennial questionnaire were asked for permission to review their medical records. Deaths were reported by next of kin or postal authorities or determined by systematic searches of the National Death Index, and permission for medical records was sought. Our group previously reported that 98% of the deaths in each cohort are ascertained.
25,26Cases of nonfatal stroke that were confirmed by letter/interview but lacked sufficient medical documentation were considered probable stroke. We considered both stroke confirmed by medical record review and probable stroke as cases in our analyses.
Ascertainment ofCHD
CHD was defined as nonfatal or fatal MI, fatal CHD, or coronary revascularization procedure (coronary artery bypass graft or percutaneous transluminal coronary angioplasty). Participants who reported an incident event on a biennial questionnaire were asked for permission to obtain medical records, which were reviewed by physicians who were blinded to the exposure status and the specifc research question under study. Nonfatal MI was confirmed according to the World Health Organization criteria, which required typical symptoms plus diagnostic electrocardiographic findings or elevated enzyme levels.
27Fatal CHD was identified by medical records or autopsy reports or if CHD was listed as the cause of death on the death certificate along with prior evidence of CHD. The study designated as probable fatal CHD deaths when no medical records surrounding the death were available, but CHD was the underlying cause on the death certificate or National Death Index search, or a family member provided supporting information on the diagnosis. Deaths were identified by report by the next of kin or the postal system or by searching the National Death Index using the methods described for stroke above.
25,26We considered both CHD confirmed by medical record review and probable CHD as cases in our analyses, as well as self‐reported revascularization procedures.
28,29
Ascertainment of Covariates
In our multivariable‐adjusted analyses, we adjusted for several factors that could potentially be related to HZ and stroke or CHD, including age, race, smoking history, body mass index, waist circumference, physical activity, medical conditions strongly related to cardiovascular risk (eg, diabetes, hypertension, and elevated cholesterol), use of aspirin, thiazide or loop diuretics, statins, and antihypertensive medication, diet quality (Alternative Healthy Eating Index 2010) score, menopausal status (women), postmenopausal hormone therapy use (women), oral contraceptive use (NHS II), family history of heart disease (defined as maternal history of MI before 65 years of age or paternal history of MI before 55 years of age), and self‐reported medical conditions that potentially compromise immunity because of disease or treatment (eg, cancer other than nonmelanoma skin cancer, rheumatoid arthritis, Crohn's disease, ulcerative colitis, systemic lupus erythematosus, asthma, diabetes, chronic obstructive pulmonary disease, and oral steroid use). Covariate information, including age, weight, physical activity, smoking status, medication use, and physician diagnosis of chronic diseases, was assessed and updated every 2 to 4 years by biennial questionnaires administered throughout follow‐up. Diet information was collected every 4 years using a validated semiquantitative food frequency questionnaire.
30,31,32,33Among the women in the NHS and NHS II, information on menopausal status, postmenopausal hormone therapy, and oral contraceptive use (NHS II only) was also obtained. Self‐reported information on height and weight was used to calculate body mass index. If covariate information was missing, we carried the information forward from up to 2 previous questionnaire cycles. The validity of covariate information collected in these cohorts has been demonstrated and is described in previous publications.
22,28,34,35
Statistical Analysis
The short‐term (up to 1 year) relation of HZ and cardiovascular disease (CVD) outcomes has been demonstrated previously.
13This study focuses on long‐term relations. The analyses were conducted using a prospective design, with information on HZ collected before the stroke or CHD event. We had information on the precise date of the CVD event, but the reporting of the date of HZ was less precise. To reduce the possibility that the CVD event preceded the episode of HZ, we censored participants who reported their HZ and had a stroke or CHD event within ±12 months. Thus, our study did not evaluate the short‐term relation of HZ and CVD. Person‐time was calculated for each participant based on the return date of the questionnaire to the diagnosis of stroke, CHD, death, or the end of follow‐up, whichever occurred first. Time (in years) since the HZ event was calculated based on the duration of the time interval from the reported diagnosis of HZ until the beginning of each 2‐year time period. HZ and covariate status were updated with each time period. We categorized time since HZ as never, 1 to 4 years since HZ, 5 to 8 years since HZ, 9 to 12 years since HZ, and ≥13 years since HZ. We used Cox proportional hazards models with time‐varying covariates and age as the underlying time scale, with stratification by calendar time (in 2‐year intervals), to estimate hazard ratios (MVHRs [95% CIs]) and assess the association between time since HZ and the subsequent risk of stroke or CHD event. In each cohort, separate analyses were conducted for risk of stroke, risk of CHD, and risk of a composite CVD outcome (a composite of stroke or CHD, whichever came first). We also performed pooled analyses for each outcome with the use of fixed‐effects meta‐analysis with inverse‐variance weighting. Heterogeneity was assessed with the I
2statistic, and low to moderate heterogeneity was observed (I
2<40%). We conducted sensitivity analyses that restricted the CHD outcome to fatal and nonfatal MI and fatal CHD events and censored those who reported coronary revascularization procedures (coronary artery bypass graft or percutaneous transluminal coronary angioplasty) during follow‐up. We also conducted stratified analyses among those with and without potentially immunocompromising health conditions, including cancer, rheumatoid arthritis, Crohn's disease, ulcerative colitis, systemic lupus erythematosus, asthma, diabetes, chronic obstructive pulmonary disease, or oral steroid use.
Results
The total study sample included 79 658 women (mean [SD] age, 65.8 [7.1] years at baseline) in the NHS (2000–2021), 93 932 women (mean [SD] age, 46.2 [4.7] years) in the NHS II (2001–2021), and 31 440 men in the HPFS (mean [SD] age, 69.5 [8.6] years) (total n=205 030). The age‐standardized characteristics of study participants according to history of HZ at a midpoint during follow‐up in each of the cohorts are shown in
Table 1(NHS: 2008; NHS II: 2009; and HPFS: 2008). Participants with a history of HZ were slightly older than those with no history of HZ, and they were slightly more likely to have conditions that could potentially compromise immunity, including cancer, rheumatoid arthritis, Crohn's disease, ulcerative colitis, systemic lupus erythematosus, asthma, chronic obstructive pulmonary disease, and oral steroid use. There were no other appreciable differences.
Table 1. Age‐Standardized Characteristics of Participants in the NHS, NHS II, and HPFS at Midpoint of Follow‐Up
(Table view)
Values are means (SDs) for continuous variables; percentages are given for categorical variables and are standardized to the age distribution of the study population. Values of polytomous variables may not sum to 100% because of rounding. AHEI indicates Alternative Healthy Eating Index; COPD, chronic obstructive pulmonary disease; HPFS, Health Professionals Follow‐Up Study; HZ, herpes zoster; METS, metabolic equivalents; NHS, Nurses' Health Study; and NHS II, Nurses' Health Study II.
*
Waist circumference assessed in 2000 (NHS), 2005 (NHS II), and 1996 (HPFS).
HZand Long‐Term Risk of Incident Stroke
During a total of 2 471 975 person‐years of follow‐up, 2461 cases of incident stroke among women in the NHS, 537 incident strokes among women in the NHS II, and 605 incident strokes among men in the HPFS were documented and included in the analysis. History of HZ was significantly and independently associated with higher long‐term risk of incident stroke (
Table 2). In pooled multivariable analyses accounting for multiple potential confounding factors, compared with individuals with no history of HZ, the MVHRs (95% CIs) for incident stroke were 1.05 (0.88–1.25) among those with 1 to 4 years since HZ, 1.38 (1.10–1.74) among those with 5 to 8 years since HZ, 1.28 (1.03–1.59) among those with 9 to 12 years since HZ, and 1.19 (0.90–1.56) among those with ≥13 years since HZ. The findings for the individual cohorts are also shown in
Table 2.
Table 2. HZ and Long‐Term Risk of Stroke in the NHS, NHS II, and HPFS
(Table view)
HPFS indicates Health Professionals Follow‐Up Study; HR, hazard ratio; HZ, herpes zoster; NHS, Nurses' Health Study; and NHS II, Nurses' Health Study II.
*
Multivariable model adjusted for age, race, family history of heart disease (yes/no), smoking history, body mass index, waist circumference (≤70, 71–79, 80–88, and >88 cm), physical activity, diabetes, hypertension, elevated cholesterol, regular use (≥2 days/week) of aspirin, thiazide diuretics, loop diuretics, “statins,” or other cholesterol‐lowering drugs, calcium‐channel blockers, β‐blockers, angiotensin‐converting enzyme inhibitors, or “other” antihypertensive drugs, Alternative Healthy Eating Index 2010 score, menopausal status (in NHS and NHS II), oral contraceptive use (in NHS II), postmenopausal hormonal therapy use (in NHS and NHS II), history of coronary heart disease, and a report of ≥1 of the following: cancer (other than nonmelanoma skin cancer), rheumatoid arthritis, Crohn's disease/ulcerative colitis (inflammatory bowel disease), systemic lupus erythematosus, asthma, diabetes, chronic obstructive pulmonary disease, or oral steroids/corticosteroid use.
HZand Long‐Term Risk of IncidentCHD
During a total of 2 350 066 person‐years of follow‐up, 4910 cases of incident CHD (nonfatal/fatal MI, fatal CHD, or coronary revascularization procedure) among women in the NHS, 1183 cases among women in the NHS II, and 2527 cases among men in the HPFS were documented and included in the analysis. History of HZ was significantly and independently associated with higher long‐term risk of CHD (
Table 3). In pooled multivariable analyses accounting for multiple potential confounding factors, compared with individuals with no history of HZ, the MVHRs (95% CIs) for incident CHD were 1.13 (1.01–1.27) among those with 1 to 4 years since HZ, 1.16 (1.02–1.32) among those with 5 to 8 years since HZ, 1.25 (1.07–1.46) among those with 9 to 12 years since HZ, and 1.00 (0.83–1.21) among those with ≥13 years since HZ. The findings for the individual cohorts are also shown in
Table 3.
Table 3. HZ and Long‐Term Risk of CHD in the NHS, NHS II, and HPFS
(Table view)
CHD indicates coronary heart disease; HPFS, Health Professionals Follow‐Up Study; HR, hazard ratio; HZ, herpes zoster; NHS, Nurses' Health Study; and NHS II, Nurses' Health Study II.
*
Multivariable model adjusted for age, race, family history of heart disease (yes/no), smoking history, body mass index, waist circumference (≤70, 71–79, 80–88, and >88 cm), physical activity, diabetes, hypertension, elevated cholesterol, regular use (≥2 days/week) of aspirin, thiazide diuretics, loop diuretics, “statins,” or other cholesterol‐lowering drugs, calcium‐channel blockers, β‐blockers, angiotensin‐converting enzyme inhibitors, or “other” antihypertensive drugs, Alternative Healthy Eating Index 2010 score, menopausal status (in NHS and NHS II), oral contraceptive use (in NHS II), postmenopausal hormonal therapy use (in NHS and NHS II), history of coronary heart disease, and a report of ≥1 of the following: cancer (other than nonmelanoma skin cancer), rheumatoid arthritis, Crohn's disease/ulcerative colitis (inflammatory bowel disease), systemic lupus erythematosus, asthma, diabetes, chronic obstructive pulmonary disease, or oral steroids/corticosteroid use.
The results from sensitivity analyses that restricted the CHD outcome to fatal and nonfatal MI and fatal CHD and censored those who reported coronary revascularization procedures are shown in Table S1. In the female cohorts, the findings were similar. However, in men, compared with those with no history of HZ, we observed a statistically significant higher risk of CHD among those with a history of HZ using the more restrictive outcome definition; compared with men with no history of HZ, the MVHR (95% CI) for incident MI was 1.36 (1.02–1.81) among those with ≥5 years since HZ.
HZand Long‐Term Risk of IncidentCVD
In analyses examining HZ and risk of a composite CVD outcome (stroke or CHD, whichever came first), previous HZ was significantly and independently associated with risk of a major cardiovascular event (
Table 4). In the pooled multivariable analyses, compared with individuals with no history of HZ, the MVHRs (95% CIs) for a cardiovascular event were 1.11 (1.01–1.23) among those with 1 to 4 years since HZ, 1.26 (1.13–1.41) among those with 5 to 8 years since HZ, 1.27 (1.11–1.46) among those with 9 to 12 years since HZ, and 1.08 (0.92–1.28) among those with ≥13 years since HZ.
Table 4also shows the findings for the individual cohorts.
Table 4. HZ and Long‐Term Risk of CVD (Composite) in the NHS, NHS II, and HPFS
(Table view)
CVD is a composite of total stroke and coronary heart disease (CHD), defined as nonfatal or fatal myocardial infarction, fatal CHD, or coronary revascularization procedure. CVD indicates cardiovascular disease; HPFS, Health Professionals Follow‐Up Study; HR, hazard ratio; HZ, herpes zoster; NHS, Nurses' Health Study; and NHS II, Nurses' Health Study II.
*
Multivariable model adjusted for age, race, family history of heart disease (yes/no), smoking history, body mass index, waist circumference (≤70, 71–79, 80–88, and >88 cm), physical activity, diabetes, hypertension, elevated cholesterol, regular use (≥2 days/week) of aspirin, thiazide diuretics, loop diuretics, “statins,” or other cholesterol‐lowering drugs, calcium‐channel blockers, β‐blockers, angiotensin‐converting enzyme inhibitors, or “other” antihypertensive drugs, Alternative Healthy Eating Index 2010 score, menopausal status (in NHS and NHS II), oral contraceptive use (in NHS II), postmenopausal hormonal therapy use (in NHS and NHS II), and a report of ≥1 of the following: cancer (other than nonmelanoma skin cancer), rheumatoid arthritis, Crohn's disease/ulcerative colitis (inflammatory bowel disease), systemic lupus erythematosus, asthma, diabetes, chronic obstructive pulmonary disease, or oral steroids/corticosteroid use.
Additional Analyses
We performed stratified analyses that compared the association of HZ and long‐term risk of stroke and CHD among those with and without potentially immunocompromising conditions. There was a suggestion that the magnitude of the elevated risk for stroke after ≥5 years since HZ was greater among women with potentially immunocompromising conditions; however, the
Pvalue for interaction was statistically significant only in the NHS II (
P‐interaction=0.05) (Table S2). In men, we did not observe that the risk varied by immune status (
P‐interaction=0.68), but the number of cases among men with a history of HZ was small. There was a suggestion that the magnitude of the risk for CHD after ≥5 years since HZ was greater among women with potentially immunocompromising conditions in the NHS II (
P‐interaction=0.03) (Table S3), but there was no evidence that the risk differed by immune status in the other 2 cohorts (
P‐interaction ≥0.2). Similarly, there was a suggestion that the magnitude of the risk for CVD (composite) after ≥5 years since HZ was greater among women with potentially immunocompromising conditions in the NHS II (
P‐interaction=0.02) but not in the other 2 cohorts (
P‐interaction ≥0.28) (Table S4).
In the male cohort, we did not have information on HZ that occurred after 2008; thus, men who had HZ after the return of the 2008 questionnaire were misclassified in the later time periods; this could have biased the results for the 1 to 4 and 5 to 8 years since HZ toward the null. When we conducted sensitivity analyses that ended follow‐up in 2010, the findings were similar.
In additional analyses that included intakes of alcohol and specific dietary factors as individual covariates, the results were not materially different (data not shown). To consider the possibility that the true effect size may differ among the cohorts, we also conducted meta‐analyses using the random effects approach. The findings were essentially unchanged.
Discussion
In 3 large cohorts of women and men with up to 16 years of follow‐up, HZ was associated with higher long‐term risk of a major adverse cardiovascular event. The higher risk persisted for 12 years and possibly longer. There was a suggestion that the magnitude of the elevated risk may be greater among those with potentially immunocompromising conditions.
Several mechanisms could underlie the observed association of HZ and long‐term risk of a major CVD event. VZV is the only human virus demonstrated to replicate in arteries and lead to vasculopathy,
11and a growing body of evidence links VZV to vascular disease.
12,13VZV has been detected in large and small blood vessels and has been implicated in the pathogenesis of several VZV‐related cardiovascular disorders.
11,14,15,16,17VZV vasculopathy develops from viral spread along nerve fibers, directly involves both intracranial and extracranial vasculature,
36,37and has been confirmed by the presence of multinucleated giant cells, herpesvirus particles, VZV DNA, and VZV antigen in arteries.
18Vascular changes associated with VZV vasculopathy, including disruption of the internal elastic lamina, intimal thickening, and reduced medial smooth muscle cells, can lead to alterations in arterial caliber and contractility,
19and vessel wall damage, arterial dissection, or aneurysm could trigger an ischemic or hemorrhagic CVD event.
11,20,36,38Notably, VZV vasculopathy may be chronic and protracted,
39and thus vascular changes could elevate risk of a CVD event years after an episode of HZ.
11Furthermore, systemic inflammation, autoimmune reactions, or hemodynamic perturbations related to HZ may also contribute to risk of a CVD event, irrespective of the site of dermatomal involvement.
12,20,21VZV‐related inflammation may also lead to endothelial dysfunction accompanied by disruption of atheromatous plaques and hypercoagulability.
37
Our study expands on prior studies by demonstrating the association between HZ and long‐term risk of stroke and CHD. Elevated risk of a major cardiovascular event within days or weeks after HZ has been reported previously.
20,38,40A comprehensive review by Wu et al summarized the findings from epidemiologic studies of HZ and risk of stroke and MI.
13Among the 15 more recent epidemiologic studies from Asia, Europe, and the United States, there was an increased incidence of stroke or MI in individuals with a recent history of HZ; the risk appeared to be highest closest to the HZ event and decreased over time.
13A meta‐analysis found higher odds of a major CVD event within 3 months of HZ onset, but whether the elevated risk persisted for more than a year was unclear.
41Notably, data on long‐term risk were limited and findings were inconsistent across studies. Most studies had limited information on health and lifestyle factors related to risk of stroke or CHD, and most were based on retrospective reviews of insurance claims or other administrative databases using diagnostic codes; thus, they captured only those individuals who sought medical attention for their HZ.
41Our study included 3 prospective cohorts with long duration of follow‐up, controlled for multiple potential confounding cardiovascular risk factors, and captured individuals whose HZ may or may not have come to medical attention, thereby providing new insight into the long‐term association of HZ and CVD.
We observed suggestive evidence of a difference in the association of HZ and risk of a major event among those with potentially immunocompromising conditions or using immunosuppressive medication in the NHS II, but not in the NHS or the HPFS. The magnitude of the elevated risk for stroke or CHD after ≥5 years since HZ was greater among NHS II women with potentially immunocompromising conditions or medication use, but there was no statistically significant evidence that the risk differed in the 2 other cohorts, so this could be a chance finding. Plausibly, reduced T‐cell immunity or other host factors could increase the risk of viral reactivation and development of vasculopathy,
42but further study of whether the association between HZ and long‐term CVD risk is modified by factors that may influence immune status is merited.
Strengths of this study include the longitudinal design, multiple independent cohorts with large sample sizes, long follow‐up with high retention rate, and repeated assessments of exposure and covariate information. Our study also has limitations. Information on HZ was self‐reported; however, it was shown to be highly reliable in the NHS. We did not have information on dermatomal involvement, treatment course, or complications, such as HZ opthalmicus; thus, future investigations that evaluate these factors could be informative. We did not have information on the date of HZ at younger ages; therefore, we were not able to examine whether the associations differed among younger individuals. We did not have information on VZV vaccination; however, we do not expect that vaccination status substantially influenced our findings. Notably, the live attenuated VZV vaccine was first recommended for individuals aged ≥60 years by the Centers for Disease Control and Prevention in 2008, a midpoint during follow‐up in our study. In 2011, expanded recommendations included individuals aged ≥50 years, but uptake was low; in 2012, uptake was 3.9% of the eligible subjects in one study
43and 20% in another.
44The more recent nonlive, recombinant subunit adjuvanted vaccine was not available until after the end of follow‐up in our study. As uptake of the VZV vaccine increases, future studies that evaluate whether vaccination status influences the relation of HZ and risk of CVD would be informative. Although we had information on specific stroke subtypes, there was not sufficient power to evaluate the associations of HZ with long‐term risk of ischemic versus hemorrhagic stroke. We controlled for several repeated measurements of diet, health, and lifestyle factors, but we cannot rule out the possibility of residual and unmeasured confounding. The generalizability of these findings may be limited because participants were predominantly non‐Hispanic White individuals.
Conclusions
A history of HZ is associated with higher long‐term risk of a major cardiovascular event. These findings suggest there are long‐term implications of HZ and underscore the importance of public health efforts for prevention.
--
We at Cross County Cardiology - Mt. Sinai, know the importance of
preventative care. The development of shingles can increase your risk of the development of long-term cardiovascular disease. Please make an appointment with our experts today. 201-299-4479 or go online to schedule an appointment today.
We recently found that the frequency of adding salt to foods could reflect a person’s long-term salt taste preference and sodium intake, and was significantly related to life expectancy.
Objective
We analyzed whether the frequency of adding salt to foods was associated with incident cardiovascular disease (CVD) risk.
Methods
This study included 176,570 adults in UK Biobank who were initially free of CVD. Cox proportional hazards models were used to estimate the association between the frequency of adding salt to foods and incident CVD events.
Results
During a median of 11.8 years of follow-up, 9,963 total CVD events, 6,993 ischemic heart disease (IHD) cases, 2,007 stroke cases, and 2,269 heart failure cases were documented. Lower frequency of adding salt to foods was significantly associated with lower risk of total CVD events after adjustment for covariates and the DASH (Dietary Approaches to Stop Hypertension) diet (a modified DASH score was used without considering sodium intake). Compared with the group of always adding salt to foods, the adjusted HRs were 0.81 (95% CI: 0.73-0.90), 0.79 (95% CI: 0.71-0.87), and 0.77 (95% CI: 0.70-0.84) across the groups of usually, sometimes, and never/rarely, respectively (Ptrend < 0.001). Among the subtypes of CVD, adding salt showed the strongest association with heart failure (Ptrend <0.001), followed by IHD (Ptrend < 0.001), but was not associated with stroke. We found that participants who combined a DASH-style diet with the lowest frequency of adding salt had the lowest CVD risk.
Conclusions
Our findings indicate that lower frequency of adding salt to foods is associated with lower risk of CVD, particularly heart failure and IHD.
-
At Cross County Cardiology - Mt. Sinai, you can count on us to inform you of all things heart related. It is because of recent studies like this one published in the journal of the American College of Cardiology that we encourage you to make an appointment to have your levels checked periodically. From one salt lover to another, please give us a call at 201-499-7361 or go online to schedule an appointment with our cardiovascular disease specialists.
At Cross County Cardiology - Mt Sinai, we are diligent in reviewing the latest findings on all things cardiology. With the recent decriminalization of marijuana, its use has continued to rise. Due to the fact that marijuana was previously illegal, significant research has been limited to certain fields like pain medicine and end of life care. However, due to its decriminalization, the amount of research into marijuana is expected to increase dramatically. While thought to be less deleterious than tobacco, it still has effects on the cardiovascular system. In fact, daily chronic marijuana users have been seen to have a slower heart rate (bradycardia) and in rare cases can even have sinus pauses/arrest.
If you or loved ones feel palpitations, lightheadedness, dizziness, or even passed out, it is important to be evaluated by a professional. Turns out MJ does have an effect on the heart. Please read these findings below to learn more. And please give us a call at 201-499-7361 or go online to schedule an appointment at one of our locations should you want to speak with one of our experts about your health.
It's official, Newsweek's latest rankings on the world's best specialized hospitals of 2022 just came out and Mount Sinai Hospital (New York City) is #4! Moreover, they showcase our passion, Cardiology! Cross County Cardiology is proud to be associated with this incredible team and institution. We're feeling blessed to be rated by Castle Connolly as NY Top Doctors and we welcome this Newsweek honor too. Check out the official list of Cardiology hospitals below.
Hypertensive disorders of pregnancy (HDP), including gestational hypertension and preeclampsia, are associated with an increased risk of CVD.
Objectives
The purpose of this study was to evaluate associations between HDP and long-term CVD and identify the proportion of the association mediated by established CVD risk factors.
Methods
Parous participants without CVD in the Nurses’ Health Study II (n = 60,379) were followed for incident CVD from first birth through 2017. Cox proportional hazards models estimated HRs and 95% CIs for the relationship between HDP and CVD, adjusting for potential confounders, including prepregnancy body mass index, smoking, and parental history of CVD. To evaluate the proportion of the association jointly accounted for by chronic hypertension, hypercholesterolemia, type 2 diabetes, and changes in body mass index, we used the difference method.
Results
Women with HDP in first pregnancy had a 63% higher rate of CVD (95% CI: 1.37-1.94) compared with women with normotensive pregnancies. This association was mediated by established CVD risk factors (proportion mediated = 64%). The increased rate of CVD was higher for preeclampsia (HR: 1.72; 95% CI: 1.42-2.10) than gestational hypertension (HR: 1.41; 95% CI: 1.03-1.93). Established CVD risk factors accounted for 57% of the increased rate of CVD for preeclampsia but 84% for gestational hypertension (bothP <0.0001).
Conclusions
Established CVD risk factors arising after pregnancy explained most (84%) of the increased risk of CVD conferred by gestational hypertension and 57% of the risk among women with preeclampsia. Screening for chronic hypertension, hypercholesterolemia, type 2 diabetes, and overweight/obesity after pregnancy may be especially helpful in CVD prevention among women with a history of HDP.
Introduction
New-onset hypertensive disorders of pregnancy (HDP) (gestational hypertension and preeclampsia) occur in approximately 15% of parous women and are consistently associated with a 2-fold increased risk of cardiovascular disease (CVD) and premature CVD-related mortality, compared with women with a history of normotensive pregnancy.1,2However, few studies of incident CVD after hypertensive pregnancies have adjusted for shared prepregnancy risk factors, such as body mass index (BMI),3-5or had a mean/median follow-up of more than 30 years.4,6-9
Women with a history of HDP have elevated risks of chronic hypertension, hypercholesterolemia, and type 2 diabetes mellitus (T2DM), and the American Heart Association and American College of Cardiology endorse preeclampsia as a risk-enhancing factor for hypercholesterolemia.10,11However, the extent to which the relationship between HDP and CVD events is mediated by these established CVD risk factors remains less clear. Previous studies have examined the role of individual mediators, but no study has examined the joint contribution of chronic hypertension, hypercholesterolemia, T2DM, and BMI in mediating the relationship between HDP and CVD.5,12,13The American Heart Association has recognized gestational hypertension and preeclampsia as risk factors for CVD and encouraged clinicians to evaluate cardiovascular risk by screening women for these adverse pregnancy outcomes since 2011.14Longitudinal investigation of CVD incidence after a hypertensive pregnancy that examines the role of intermediate CVD risk factors is essential to inform screening practices and clinical recommendations for women with a history of HDP.
With up to over 50 years of follow-up after first birth and longitudinal collection of health-related behaviors, reproductive history, and incident CVD risk factors and events, we examined the association between HDP and CVD, controlling for prepregnancy confounders, and examined mediation by subsequent CVD risk factors—chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI—in the NHSII (Nurses’ Health Study II).
Methods
Cohort description
The NHSII is an ongoing cohort of 116,429 female U.S. registered nurses aged 25-42 years at enrollment in 1989. Participants are followed prospectively through biennial questionnaires, which ascertain information on health-related behaviors, medication use, and incident disease. The average active follow-up rate for each questionnaire is >90%. This study protocol was approved by the Institutional Review Boards of Brigham and Women’s Hospital and the Harvard T.H. Chan School of Public Health (protocol number: 1999P003389).
Hypertensive disorders of pregnancy
The 2009 biennial questionnaire captured complete pregnancy history, including adverse pregnancy outcomes and gestation length. Participants self-reported HDP as “pregnancy-related high blood pressure” (gestational hypertension) or “preeclampsia/toxemia.” Since this questionnaire did not ascertain chronic hypertension during pregnancy, the analysis focused on new-onset hypertension in pregnancy (gestational hypertension and preeclampsia). A validation study among 462 NHSII participants who self-reported preeclampsia on biennial questionnaires from 1991 to 2001 demonstrated that 89% had medical record evidence of preeclampsia.10The primary analysis focused on HDP in first pregnancy (normotension [ref], gestational hypertension, preeclampsia) because HDP predominantly occurs during first pregnancies15and to avoid potential bias induced by selective fertility (wherein the decision to pursue subsequent pregnancies is dependent on previous pregnancy outcomes).16A secondary analysis examined HDP exposure across all lifetime pregnancies, including ever and recurrent HDP (see theSupplemental Appendixfor details).
CVD events
Participants reported history of physician-diagnosed “myocardial infarction (MI) or angina” or “stroke (cerebrovascular accident) or transient ischemic attack” on the 1989 baseline questionnaire. Subsequent biennial questionnaires captured incident CVD events. Participants or next of kin approved medical record access for validation of incident events. MI events were confirmed using the World Health Organization criteria of symptoms plus either diagnostic electrocardiographic results or elevated cardiac-specific enzymes.17,18Fatal coronary artery disease (CAD) events were confirmed using hospital records, autopsy, or death certificates among individuals with evidence of prior CAD. Stroke was confirmed using National Survey of Stroke criteria, requiring neurological deficit with rapid or sudden onset that persisted for >24 hours or until death.19Strokes discovered through radiological imaging alone and cerebrovascular pathology resulting from infection, trauma, or malignancy (“silent” strokes) were not included. CVD events, including CAD (MI or fatal CAD) and stroke, that satisfied these criteria upon medical record review were considered definite. CVD events for which medical records could not be obtained or for which permission was not granted but were confirmed by the participant or a relative were considered probable. Definite and probable CVD cases comprised the outcome of interest.
Covariates
In 1989, participants reported race/ethnicity, current height and weight, weight at age 18 years, physical activity, parental history of MI before age 60 years, medical history (including chronic hypertension and diabetes not during pregnancy), and history of smoking, alcohol consumption, and oral contraceptive use. Biennial questionnaires after 1989 updated health-related behaviors and additionally ascertained diet, an expanded personal medical history (including hypercholesterolemia), and the nurse’s parents’ education level, history of stroke before age 60 years, and ages at and causes of death.
BMI (kg/m2) was calculated from height and weight at age 18 years and at each biennial questionnaire. For ages at which weight was not reported, BMI was derived based on reported weights and incorporating somatograms at ages 20, 30, and 40 years.10Diet was summarized in quintiles using the 2010 Alternative Healthy Eating Index dietary quality score, derived from food frequency questionnaires.20Self-reported weight at age 18 years, current height, diet, and physical activity have been shown to be reliable in previous validation studies (see theSupplemental Methods). Prepregnancy information was drawn from the biennial questionnaire immediately before the first pregnancy. Because most first pregnancies (83%) occurred before NHSII enrollment, information about health-related behavior in high school and within varying age ranges from 13 through 42 years reported at baseline was used to assign prepregnancy values for women with first births before 1989.
Hypercholesterolemia was defined as self-report of hypercholesterolemia or cholesterol-lowering medication use (collected since 1999). Incident diabetes was confirmed through a supplemental questionnaire, which collected information on symptoms, diagnostic tests, and treatment. Diabetes cases were classified into categories established by the National Diabetes Data Group and American Diabetes Association, as described elsewhere.21-23Participants reported the year of diagnosis for incident physician-diagnosed conditions within 3 categories. For chronic hypertension and hypercholesterolemia, the midpoint of each date range was used as the year of diagnosis. For T2DM, year of diagnosis came from the supplemental questionnaire. Medical record validation has previously demonstrated the accuracy of nurse participants’ self-report of chronic hypertension (sensitivity: 94%), hypercholesterolemia (confirmation: 86%), and T2DM (confirmation: ≥98%).24-26
Exclusions
Analyses were restricted to women who completed the 2009 biennial questionnaire, which permitted dating of first birth and assignment of HDP exposure (n = 76,840). After applying additional exclusion criteria (Figure 1), 60,379 parous women free of CVD before first pregnancy were retained in the primary analysis. For the mediation analysis, we further restricted to 57,974 women at risk for the potential mediators of interest. The analysis of lifetime HDP started follow-up at age 40 years (by which point 95% of women had experienced their final pregnancy) and was restricted to 57,137 parous women with their final pregnancy before age 40 years and who remained free of CVD at age 40 years.
Figure 1
Flow Diagram for the Primary, Mediation, and Secondary Analyses
∗Women reporting chronic hypertension within 1 year after first birth (n = 115) were excluded to prevent misclassification of exposure (undetected chronic hypertension before pregnancy may be incorrectly captured as incident chronic hypertension directly following pregnancy) and because the exact date of diagnosis was unknown, which prevented definitive determination as to whether the chronic hypertension arose before, during, or after pregnancy. CVD = cardiovascular disease; HDP = hypertensive disorders of pregnancy.
Statistical analysis
Characteristics of the analytic population at first pregnancy and at 1989 NHSII enrollment were standardized to the age distribution of the population and summarized by HDP status in first pregnancy (Table 1). Cox proportional hazards models estimated HRs and 95% CIs for the association between HDP and CVD. Women contributed person-time to the analysis from first birth until confirmed CVD, death, last returned questionnaire, or 2017 (Figure 2).
Table 1 Age-Standardized Characteristics of Nurses’ Health Study II Participants by Hypertensive Status at First Pregnancy
Hypertensive Disorder in First Pregnancy Status
Normotensive Pregnancy (n = 54,756, 90.7%)
Gestational Hypertension (n = 1,789, 3.0%)
Preeclampsia (n = 3,834, 6.4%)
Age at first birth, ya
27.0 ± 4.6
28.2 ± 4.9
27.0 ± 4.8
Age at NHSII enrollment (1989), ya
35.1 ± 4.7
34.3 ± 4.7
34.5 ± 4.6
Nulliparous at NHSII enrollment
16
18
16
Race/ethnicity
White
94
95
94
Black
1
1
1
Hispanic/Latina
2
1
2
Asian
1
1
1
Other/Multiracial
2
2
2
Participant mother’s education >12 y
32
32
32
Participant father’s education >12 y
38
35
38
Strenuous physical activity, at ages 18-22 y
Never
28
29
27
10-12 months/y
11
11
11
Prepregnancy body mass index, kg/m2
21.8 ± 3.5
23.3 ± 4.4
22.9 ± 4.2
Prepregnancy body mass index ≥30 kg/m2
2
7
6
Prepregnancy type 2 diabetes mellitusb
<1
0
0
Prepregnancy hypercholesterolemia
3
3
4
Parental history of MI/fatal CAD or stroke before age 60 y
20
24
24
Alternative Healthy Eating Index scorec
Lowest quintile (unhealthy)
20
23
22
Highest quintile (healthy)
19
20
18
Prepregnancy smoking status
Never
68
70
68
Past
10
9
10
Current
22
21
22
Prepregnancy alcohol intake
None
26
27
28
≤1 drink/wk
37
36
36
2-6 drinks/wk
29
29
28
≥1 drink/d
8
8
8
Prepregnancy oral contraceptive use
Never
22
21
19
<2 y
25
26
27
2-<4 y
22
21
22
≥4 y
31
32
32
Preterm delivery (<37 wks) in first birth
8
8
16
Final parityd
1 birth
16
21
22
2 births
49
48
49
3 births
26
23
23
≥4 births
9
8
7
Figure 2
Nurses’ Health Study II Data Collection Timeline and Analytic Follow-Up
Ascertainment of exposure and assignment of prepregnancy covariate information for participants with their first birth before cohort enrollment and for those with their first birth during active follow-up. CVD = cardiovascular disease.
We compared the distributions of age at and time to CVD development between HDP groups using log-rank tests. Multivariable models were adjusted for variables identified a priori as prepregnancy confounding variables: age at first birth; age at NHSII enrollment; race/ethnicity; parental education; strenuous physical activity at ages 18-22 years; parental history of CVD before age 60 years; and prepregnancy BMI, alcohol consumption, diet, smoking, oral contraceptive use, and hypercholesterolemia. (As only 11 women developed T2DM before first pregnancy, this was not included in multivariable adjustment.) Models for lifetime HDP additionally adjusted for final parity. Missing covariate data were addressed by missing indicators. To evaluate nonlinear departures from proportional hazards, we used restricted cubic splines to conduct a nonparametric test of whether the HDP-CVD association was modified by time since first birth.27,28As no nonlinearity was revealed, we tested for linear departures through a likelihood ratio test, comparing nested models with and without multiplicative interaction terms between the following: 1) gestational hypertension and time since first birth; and 2) preeclampsia and time since first birth; no linear departures from proportional hazards were found(P =0.12). Multivariable-adjusted cumulative incidence curves for CVD were obtained at the mean and mode values of the continuous and categorical covariates, respectively, using the Breslow estimator.
To evaluate chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI occurring after first pregnancy as potential mediators, we used the difference method, fitting models with and without these established CVD risk factors.29Chronic hypertension, hypercholesterolemia, and T2DM were treated as time-dependent binary mediators and, once a woman developed a mediator, she was considered to have the mediator through end of follow-up. BMI was treated as a time-varying continuous mediator, updated over follow-up according to self-reported changes in weight. Mediation analysis requires the following assumptions: 1) no unmeasured exposure-outcome confounding; 2) no unmeasured mediator-outcome confounding; 3) no unmeasured exposure-mediator confounding; and 4) no mediator-outcome confounder affected by the exposure.30To control for confounding of these relationships, we additionally adjusted for updated behaviors over follow-up in mediation models. We tested for the presence of interactions between each mediator and HDP using likelihood ratio tests of nested models with and without the interactions; no exposure-mediator interactions were found (allP> 0.05). We used the SAS %mediate macro to calculate the proportion of the HDP-CVD jointly mediated by chronic hypertension, T2DM, hypercholesterolemia, and BMI.31,32Several sensitivity analyses were conducted to examine the robustness of our findings (Supplemental Appendix). All analyses were conducted using SAS 9.4 (SAS Institute, Inc).
Results
Approximately 10% of women experienced HDP in their first pregnancy. First births occurred between 1964 and 2008 at an average age of 27.0 ± 4.7 years. Women with HDP in first pregnancy were similar to those with normotensive first pregnancies in demographics and health-related behaviors (Table 1). However, women with HDP were >3 times as likely to have a prepregnancy BMI ≥30 kg/m2and were more likely to have a parent with a premature CVD event.
By the end of follow-up, when participants were a median age of 61 years (IQR: 57-64 years; range 33-71 years) with a median follow-up of 34 years since first birth (IQR: 29-40 years; range 2-54 years), 1,074 (1.8%) women had experienced a first CVD event—560 CAD events (554 MIs and 6 fatal CAD) and 515 strokes (n = 1 woman had both an MI and stroke). In fully adjusted models, women with HDP in first pregnancy had a 63% increased rate of CVD compared with women with a normotensive first pregnancy (95% CI: 1.4-1.9) (Table 2, Model 2). Adjustment for prepregnancy BMI, smoking, and parental history of CVD accounted for most of the modest attenuation between age, race/ethnicity, and parental education-adjusted and fully adjusted estimates. When we separately examined gestational hypertension and preeclampsia with CAD and stroke endpoints, there were significant associations between preeclampsia and CAD (HR: 2.2; 95% CI: 1.7-2.8) and gestational hypertension and stroke (HR: 1.6; 95% CI: 1.0-2.4) (Central Illustration). Further adjustment for updated smoking, diet, alcohol intake, physical activity, and oral contraceptive use after pregnancy resulted in slight attenuation but did not alter conclusions (data not shown). Women with HDP in first pregnancy exhibited elevated rates of CVD relative to women with normotensive first pregnancies, regardless of gestation length (Table 3).
Table 2 Hypertensive Disorders in First Pregnancy and Cardiovascular Disease
Hypertensive Disorder in First Pregnancy Status
Normotensive Pregnancy (n = 54,756, 90.7%)
Gestational Hypertension (n = 1,789, 3.0%)
Preeclampsia (n = 3,834, 6.4%)
Hypertensive Disorders of Pregnancy (n = 5,623, 9.3%)
CVD (CAD or stroke)
Cases/person-y
920/1,885,474
41/57,900
113/128,840
154/186,740
Excess cases per 100,000 person-y
—
22
39
34
Median age at event (IQR), ya
56 (50-62)
58 (52-63)
55 (47-60)
56 (48-62)
Median time to event (IQR), ya
35 (29-40)
32 (27-37)
34 (29-39)
33 (28-38)
Model 1
1.00 (ref)
1.55 (1.13-2.12)
1.87 (1.54-2.28)
1.78 (1.50-2.11)
Model 2
1.00 (ref)
1.41 (1.03-1.93)
1.72 (1.42-2.10)
1.63 (1.37-1.94)
CAD
Cases/person-y
467/1,831,185
19/56,130
74/125,080
93/181,210
Excess cases per 100,000 person-y
—
8
34
26
Median age at event (IQR), ya
56 (51-61)
61 (55-65)
55 (47-61)
57 (50-62)
Median time to event (IQR), ya
34 (28-39)
31 (26-36)
33 (28-38)
32 (27-37)
Model 1
1.00 (ref)
1.42 (0.90-2.25)
2.42 (1.90-3.10)
2.12 (1.70-2.65)
Model 2
1.00 (ref)
1.27 (0.80-2.02)
2.21 (1.73-2.84)
1.93 (1.54-2.41)
Stroke
Cases/person-y
454/1,831,172
22/56,133
39/125,045
61/181,178
Excess cases per 100,000 person-y
—
14
6
9
Median age at event (IQR), yb
57 (50-62)
56 (52-62)
54 (48-60)
55 (48-61)
Median time to event (IQR), yb
34 (28-39)
31 (26-36)
33 (28-38)
32 (27-37)
Model 1
1.00 (ref)
1.67 (1.09-2.56)
1.29 (0.93-1.80)
1.41 (1.08-1.84)
Model 2
1.00 (ref)
1.56 (1.01-2.40)
1.21 (0.87-1.68)
1.32 (1.00-1.73)c
Central Illustration
Differential Associations by Hypertensive Disorder of Pregnancy and Cardiovascular Disease Subtypes
HRs and 95% CIs were obtained from fully adjusted Cox proportional hazards models (
Table 2, Model 2). The overall association between having a hypertensive disorder in first pregnancy and long-term maternal cardiovascular disease appeared to be driven by underlying associations between preeclampsia and coronary artery disease and between gestational hypertension and stroke.
Table 3 Hypertensive Disorders in First Pregnancy and Cardiovascular Disease by Gestation Length
CVD (CAD or Stroke)
HDP and Gestational Length at Delivery Status
Term (≥37 wks)
Preterm (<37 wks)
Normotensive Pregnancy (n = 50,404, 83.5%)
Gestational Hypertension (n = 1,643, 2.7%)
Preeclampsia (n = 3,216, 5.3%)
HDP (n = 4,859, 8.1%)
Gestational Hypertension (n = 146, 0.2%)
Preeclampsia(n = 618, 1.0%)
HDP (n = 764, 1.3%)
Cases/person-y
820/1,737,169
40/53,413
95/109,544
135/162,957
1/4,487
18/19,296
19/23,783
Excess cases per 100,000 person-y
—
28
40
36
a
46
33
Model 1
1.00 (ref)
1.69 (1.23-2.33)
1.89 (1.53-2.34)
1.83 (1.52-2.19)
a
2.21 (1.39-3.53)
1.88 (1.19-2.96)
Model 2
1.00 (ref)
1.53 (1.11-2.11)
1.74 (1.40-2.15)
1.67 (1.39-2.01)
a
2.04 (1.27-3.25)
1.74 (1.10-2.75)
Women with HDP in first pregnancy also developed CVD slightly younger and sooner after their first birth than women with normotensive first pregnancies (Table 2). The increased rate of CVD among women with HDP in first pregnancy became statistically significant between 40-49 years of age, ranging between a 41% and 81% increased rate through age 69 years (Supplemental Table 1). Women with HDP exhibited a higher cumulative incidence of CVD that emerged approximately 10 years after first birth for women with preeclampsia and 30 years after first birth for women with gestational hypertension (Figure 3).
Figure 3
Multivariable-Adjusted Cumulative Incidence of Cardiovascular Disease
Curves were obtained at the mean and mode values of the following continuous and categorical covariates, respectively: age at first birth; age at Nurses’ Health Study II enrollment; race/ethnicity; parental education; physical activity at ages 18-22 years; parental history of cardiovascular disease age <60 years; and prepregnancy smoking, body mass index, alcohol consumption, Alternative Healthy Eating Index score, oral contraceptive use, and hypercholesterolemia.
In total, 12% of women experienced at least 1 lifetime pregnancy characterized by HDP, and 2.2% (n = 1,265) experienced recurrent HDP (Table 4). Ever experiencing HDP was associated with a 63% higher rate of CVD (95% CI: 1.4-1.9) compared with women without HDP(Table 4, Model 3). Women with 1 pregnancy complicated by HDP had a 48% higher rate of CVD (95% CI: 1.2-1.8), and women with 2 or more HDP pregnancies had a 2.3-fold higher rate (95% CI: 1.7-3.1) compared with women with all normotensive pregnancies. Women with a history of 1 or more HDP pregnancies exhibited higher rates of CVD regardless of which pregnancies were complicated by HDP, although the highest relative risk was observed among women with recurrent HDP that affected their first and then a second or later pregnancy (HR: 2.5; 95% CI: 1.8-3.3).
Table 4 Ever and Recurrent Hypertensive Disorders of Pregnancy and Cardiovascular Disease
Pregnancy History at Age 40 y
n (%)
Cases/Person-y
HR (95% CI)
Model 1
Model 2
Model 3
Ever HDPa
6,639 (11.6)
180/137,586
1.78 (1.52-2.10)
1.63 (1.38-1.92)
1.63 (1.39-1.92)
Number of HDP Pregnancies
0
50,498 (88.4)
824/1,084,133
1.00 (ref)
1.00 (ref)
1.00 (ref)
1
5,374 (9.4)
132/111,825
1.61 (1.34-1.94)
1.48 (1.23-1.79)
1.48 (1.23-1.78)
2+
1,265 (2.2)
48/25,761
2.53 (1.89-3.39)
2.26 (1.68-3.04)
2.28 (1.70-3.07)
First Pregnancy
Second or Later Pregnancies
Normotensive
All Normotensive
42,397 (74.2)
670/906,026
1.00 (ref)
1.00 (ref)
1.00 (ref)
Normotensive
No Further Pregnancies
8,101 (14.2)
154/178,107
1.25 (1.04-1.49)
1.19 (0.99-1.42)
1.15 (0.96-1.39)
Normotensive
Any HDP
1,336 (2.3)
38/28,147
1.80 (1.30-2.50)
1.65 (1.19-2.29)
1.67 (1.20-2.32)
HDP
All Normotensive
2,979 (5.2)
63/61,140
1.46 (1.13-1.89)
1.36 (1.05-1.77)
1.36 (1.05-1.76)
HDP
No Further Pregnancies
1,178 (2.1)
33/24,957
2.01 (1.41-2.85)
1.76 (1.23-2.51)
1.71 (1.20-2.45)
HDP
Any HDP
1,146 (2.0)
46/23,342
2.78 (2.06-3.74)
2.45 (1.81-3.32)
2.45 (1.81-3.31)
Comparing models for HDP and CVD with and without CVD risk factors developing after pregnancy, 63.8% (95% CI: 38.6%-83.2%;P <0.0001) of the association between HDP in first pregnancy and CVD was jointly mediated by the subsequent development of chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI (Table 5). The proportion mediated (PM) by these factors was higher for gestational hypertension (PM = 83.8%) than preeclampsia (PM = 57.3%). All CVD risk factors contributed to mediation; however, chronic hypertension accounted for the largest individual proportion followed by changes in BMI, hypercholesterolemia, and T2DM. Chronic hypertension individually mediated 81% and 48% of the associations between gestational hypertension and preeclampsia with CVD, respectively. Among women with CVD events, 95% of those with gestational hypertension (n = 39 of 41) and 89% of those with preeclampsia (n = 101 of 113) developed chronic hypertension between first pregnancy and their CVD event.
Table 5 Mediation of the HDP-CVD Relationship by Chronic Hypertension, Hypercholesterolemia, Type 2 Diabetes, and BMI Changes
Hypertensive Disorder in First Pregnancy Status
Normotensive Pregnancy (n = 52,668, 90.9%)
Gestational Hypertension (n = 1,675, 2.9%)
Preeclampsia (n = 3,631, 6.3%)
Hypertensive Disorders of Pregnancy (n = 5,306, 9.2%)
Cases/person-y
752/1,676,801
37/50,326
95/112,328
132/162,654
Without mediators (total effect)
1.00 (ref)
1.52 (1.09-2.12)
1.73 (1.24-2.42)
1.67 (1.38-2.01)
With mediators (direct effect)a
1.00 (ref)
1.07 (0.77-1.49)
1.26 (0.90-1.77)
1.20 (1.00-1.45)
Proportion mediatedb(95% CI)
Ref
83.8% (3.6%-99.9%)
57.3% (24.2%-84.9%)
63.8% (38.6%-83.2%)
Individually mediated by:
Chronic hypertension
Ref
80.7% (6.1%-99.6%)
48.0% (21.9%-75.3%)
56.2% (35.2%-75.1%)
Hypercholesterolemia
Ref
19.2% (8.0%-39.2%)
15.3% (8.0%-27.4%)
16.2% (10.9%-23.4%)
Type 2 diabetes mellitus
Ref
13.1% (5.3%-29.0%)
9.1% (4.4%-18.0%)
10.1% (6.3%-15.7%)
Changes in BMI
Ref
30.4% (12.1%-58.1%)
23.0% (11.8%-40.2%)
24.8% (16.3%-35.8%)
Sensitivity analyses
Sensitivity analyses to address the potential for outcome misclassification, immortal person-time bias, survival bias, and unmeasured confounding, and to examine an alternative method for handling missing data (multiple imputation by chained equations) did not materially alter the results (Supplemental Appendix,Supplemental Tables 2 and 3).
Discussion
Women with HDP in first pregnancy had a 63% higher rate of future CVD events compared with women with normotension, even after accounting for important shared risk factors, including prepregnancy BMI, smoking, and parental history of CVD. This elevated rate was largely explained by subsequent development of established CVD risk factors—chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI—in the years after a hypertensive first pregnancy. The HDP-CVD relationship appeared to be driven by associations between preeclampsia and CAD and between gestational hypertension and stroke.
This study deepens our understanding of the relationship between HDP and long-term maternal CVD and highlights targets for potential risk reduction. Previous studies, largely unadjusted for prepregnancy cardiometabolic confounding factors, suggested an increased CVD risk of 1.7- to 2.7-fold in women with a history of HDP, depending on the specific exposure and outcome of interest, length of follow-up, and degree of adjustment.1The longitudinal nature of the NHSII permitted thorough adjustment for prepregnancy risk factors; yet, inclusion of prepregnancy demographic and behavioral variables only slightly attenuated HRs for the relationship between HDP and CVD. We found that 64% of the increased CVD risk associated with HDP was explained by subsequent development of chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI. The fact that chronic hypertension accounted for much of this association is consistent with previous mediation analyses.5,12,13For example, an analysis among 220,024 women with a mean age of 57 years at baseline and followed for a median of 7 years in the UK Biobank found that chronic hypertension accounted for 64% of the increased risk of CAD among women with a history of HDP.13The large degree of mediation observed in the HDP-CVD relationship may also partially explain why including HDP in an established CVD risk score does not appear to improve CVD prediction in women ≥40 years of age.33
NHSII participants were followed for a median of 34 years after first birth and provided a complete reproductive history, which allowed examination of CVD risk associated with HDP exposure in any pregnancy. Although history of HDP in any pregnancy increased a woman’s risk of CVD relative to women without HDP, recurrent HDP in 2 or more pregnancies was associated with a more than doubling of CVD risk—findings consistent with those from the Swedish Medical Birth Register.34
Much of the previous literature has focused on preeclampsia or examined the hypertensive disorders jointly; with >60,000 parous women, we were able to examine gestational hypertension and preeclampsia separately, yielding informative differential relationships. Women with a history of preeclampsia in first birth had an increased rate of CAD but not stroke, whereas the opposite was true for women with a history of gestational hypertension, which conferred an increased rate of stroke but not CAD. This finding is consistent with a growing understanding that the HDP subtypes may represent different disease phenotypes rather than a spectrum of severity. The suggestion that gestational hypertension might be more strongly linked to stroke than preeclampsia in our data is consistent with findings from the Northern Finland Birth Cohort 1966.4Further, our mediation findings demonstrated that chronic hypertension accounted for a greater proportion of the association between gestational hypertension and CVD than that between preeclampsia and CVD, and we previously found women with gestational hypertension to have a higher risk of developing chronic hypertension than women with preeclampsia.10Given these findings and the primacy of hypertension as a risk factor for stroke,35it is not surprising to see the association between gestational hypertension and stroke in the current analysis.
Although gestational hypertension appears to be a pure hypertensive phenotype, the pathophysiology underlying preeclampsia is more heterogeneous, stemming from abnormal placentation that results in endothelial dysfunction, systemic vascular impairment, vasoconstriction, and end-organ ischemia during pregnancy.36In the years and decades following delivery, women with a history of preeclampsia exhibit vascular endothelial dysfunction, changes to cardiac structure and function, and increased premature vascular aging and subclinical atherosclerosis.36-41Endothelial dysfunction may serve as a shared risk factor for both preeclampsia and CAD via inadequate vascularization of the uterus during pregnancy and of the myocardium later in life.40
Study limitations
The primary study limitation is the potential for exposure misclassification, given nurse participants’ self-reported HDP. However, an NHSII validation study confirmed medical record evidence of preeclampsia for the majority of women who reported it. Although HDP additionally includes chronic hypertension and superimposed preeclampsia,42this analysis focused on new-onset hypertension during pregnancy (gestational hypertension and preeclampsia), which is consistent with existing HDP-CVD literature.1Although we cannot rule out the potential for residual or unmeasured confounding (such as by social determinants of health), this study provides the most complete prepregnancy covariate adjustment currently available. Further, based on the calculated E-values, an unmeasured confounder would need to be associated with both HDP and CVD by a magnitude of 2.0- to 3.9-fold above and beyond the measured variables included in the model to explain away the observed associations. The only measured confounder within that range was prepregnancy obesity (HR: 2.4; Model 2 for HDP-CVD), so it is unlikely that the observed associations were caused by an unmeasured confounder. Finally, NHSII participants are predominantly White nurses, and our findings should be generalized to other populations with some caution. In particular, non-Hispanic Black women have higher risks of HDP and CVD, relative to non-Hispanic White women, and rates of preeclampsia are increasing more rapidly among Black women than White women43; yet, it remains to be seen whether the magnitude of the HDP-CVD association differs among these and other women of color.
Women who develop HDP typically exhibit a subtle adverse cardiovascular risk profile before pregnancy, as demonstrated in this and previous studies.44Although this suggests the CVD risk trajectory precedes pregnancy, the experience of HDP itself may also induce vascular, endothelial, or organ damage that directly increases a woman’s risk of CVD.45,46However, regardless of whether the HDP-CVD relationship is causal, HDP has the potential to be a powerful clinical risk marker. The “stress test” of pregnancy may help alert women and their providers to their underlying cardiovascular risk, creating an opportunity for primordial prevention of CVD risk factors.43,47,48To leverage this window of opportunity, however, bridges need to be established between obstetric and primary care for risk communication, behavioral intervention, and follow-up; primary care providers and cardiologists should also be sure to obtain reproductive histories from their patients.
Conclusions
To our knowledge, this study presents the most complete control of prepregnancy confounding in the relationship between HDP and long-term CVD and is the first to estimate the proportion of this association jointly mediated by chronic hypertension, hypercholesterolemia, T2DM, and changes in BMI. Even after adjustment for prepregnancy confounders, HDP in first pregnancy remained associated with a 63% higher rate of CVD later in life. Over 80% of the increased risk of CVD among women with gestation hypertension was accounted for by the development of chronic hypertension after pregnancy. Although the majority of the preeclampsia-CVD association was jointly explained by established CVD risk factors, approximately 40% of the association remained unexplained; this suggests that preeclampsia may increase the risk of CVD through nontraditional and/or under-recognized risk factors. Our findings suggest that screening for and treatment of chronic hypertension, hypercholesterolemia, T2DM, and overweight/obesity following a pregnancy may delay, or even prevent, cardiovascular disease among women with a history of HDP.
--
At Cross County Cardiology - Mt. Sinai, we strive to keep you healthy, not only now, but in your future too. And as it pertains to our female patients looking ahead to the birth a child(s), it's very important to us that both you and your baby are doing what you can to minimize hypertension during pregnancy. This is why we asked Dr. Christopher Pumill to give us his input on this article.
Dr. Christopher Pumill says, "Women who have hypertensive disorders during pregnancy (ex: gestational hypertension, pre-eclampsia, eclampsia) is associated development of cardiovascular disease long-term. In fact, women who had a hypertensive pregnancy disorder had a 60% increase in risk of developing cardiovascular disease than normotensive patients. In the setting of this increased risk, its prudent to closely monitor and manage all other traditional risk factors of CVD (hypertension, high cholesterol, diabetes, metabolic syndrome, etc)."
So take it from the best heart experts in NJ and make sure to closely monitor both you and your baby's health. If you're feeling any symptoms, please just give us a call at 201-499-7361. We're here with you all the way!
Going on a low-carb diet has long been a popular weight loss strategy. But some doctors and nutrition experts have advised against doing so over fears that it could increase the risk of heart disease, since such diets typically involve eating lots of saturated fats, the kind found in red meat and butter.
But a new study, one of the largest and most rigorous trials of the subject to date, suggests that eating a diet low in carbohydrates and higher in fats may be beneficial for your cardiovascular health if you are overweight.
The new study, which waspublished in the American Journal of Clinical Nutrition, found that overweight and obese people who increased their fat intake and lowered the amount of refined carbohydrates in their diet — while still eating fiber-rich foods like fresh fruits, vegetables, nuts, beans and lentils — had greater improvements in their cardiovascular disease risk factors than those who followed a similar diet that was lower in fat and higher in carbs. Even people who replaced “healthy” whole grain carbs like brown rice and whole wheat bread with foods higher in fat showed striking improvements in a variety of metabolic disease risk factors.
The study suggests that eating fewer processed carbs while eating more fat can be good for yourheart health, said Dr. Dariush Mozaffarian, a cardiologist and dean of the Friedman School of Nutrition Science and Policy at Tufts University, who was not involved with the research. “I think this is an important study,” he said. “Most Americans still believe that low-fat foods are healthier for them, and this trial shows that at least for these outcomes, the high-fat, low-carb group did better.”
Still, Dr. Mozaffarian stressed, the types and balance of fats you eat also appear to be important. People on the low-carb diet consumed foods like butter, red meat and whole milk, which are rich in saturated fats. But most of the fat in their diets — about two thirds — was unsaturated, which is the kind of fat that is predominantly found in olive oil, avocados, nuts, seeds and fish.
“It’s a well controlled trial that shows that eating lower carb and more saturated fat is actually good for you, as long as you have plenty of unsaturated fats and you’re mostly eating a Mediterranean-type diet,” Dr. Mozaffarian added. Many doctors recommend a traditional Mediterranean style diet, rich in fruits and vegetables, fish and heart-healthy fats like nuts and olive oil, for cardiovascular health.Other rigorous studieshave found that following a Mediterranean diet can help to ward off heart attacks and strokes.
The new study included 164 overweight and obese adults, mostly women, and took part in two phases. First, the participants were put on strict, low-calorie diets that lowered their body weights by about 12 percent. Then they were each assigned to follow one of three diets in which 20 percent, 40 percent or 60 percent of their calories came from carbohydrates.
Protein was kept steady at 20 percent of calories in each diet, with the remaining calories coming from fat. The participants were fed just enough calories to keep their weights stable. The participants followed the eating plans for five months, with all of their meals provided to ensure that they stuck to their diets.
The average Americangets about 50 percent of his or her daily caloriesfrom carbs, most of them in the form of highly processed starchy foods like pastries, bread and doughnuts and sugary foods and beverages. In the new study, the low-carb group ate significantly fewer carbs than the average American. But they were not on a super-low-carb ketogenic diet, which severely restricts carbs to less than 10 percent of daily calories and forces the body to burn fat rather than carbohydrates. Nor did they eat unlimited amounts of foods high in saturated fats like bacon, butter and steak.
Instead, the researchers designed what they considered practical and relatively healthy diets for each group. All of the participants ate meals like vegetable omelets, chicken burritos with black beans, seasoned London broil, vegetarian chili, cauliflower soup, toasted lentil salads and grilled salmon. But the high-carb group also ate foods like whole wheat bread, brown rice, multigrain English muffins, strawberry jam, pasta, skim milk and vanilla yogurt. The low-carb group skipped the bread, rice and fruit spreads and sugary yogurts. Instead, their meals contained more high-fat ingredients such as whole milk, cream, butter, guacamole, olive oil, almonds, peanuts, pecans and macadamia nuts, and soft cheeses.
After five months, people on the low-carb diet did not experience any detrimental changes in their cholesterol levels, despite getting 21 percent of their daily calories from saturated fat. That amount is more than doublewhat the federal government’s dietary guidelines recommend. Their LDL cholesterol, the so-called bad kind, for example, stayed about the same as those who followed the high-carb diet, who got just 7 percent of their daily calories from saturated fat. Tests also showed that the low-carb group had a roughly 15 percent reduction in their levels of lipoprotein(a), a fatty particle in the blood that isstrongly linked to the development of heart disease and strokes.
The low-carb group also saw improvements in metabolic measures linked to the development of Type 2 diabetes. The researchers assessed their lipoprotein insulin resistance scores, or LPIR, a measure of insulin resistance that looks at the size and concentration of cholesterol-carrying molecules in the blood.Large studies have foundthat people with high LPIR scores are more likely to develop diabetes. In the new study, people on the low-carb diet saw their LPIR scores drop by 15 percent — reducing their diabetes risk — while those on the high-carb diet saw their scores rise by 10 percent. People on the moderate carb diet had no change in their LPIR scores.
The low-carb group had other improvements as well. They had a drop in their triglycerides, a type of fat in the blood that is linked to heart attacks and strokes. And they had increases in their levels of adiponectin, a hormone that helps to lower inflammation andmake cells more sensitive to insulin, which is a good thing. High levels of body-wide inflammation are linked to a range of age-related illnesses, including heart disease and diabetes.
The low-carb diet that was used in the study largely eliminated highly processed and sugary foods while still leaving room for “high quality” carbs from whole fruits and vegetables, beans, legumes and other plants, said Dr. David Ludwig, an author of the study and an endocrinologist at Harvard Medical School. “It’s mainly focused on eliminating the processed carbs, which many people are now recognizing are among the least healthful aspects of our food supply,” said Dr. Ludwig, who is co-director of the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital.
Dr. Ludwig stressed that the findings do not apply to the very-low carb levels typical of ketogenic diets, whichhave been shown to cause sharp elevationsin LDL cholesterol in some people. But he said the study does show that people can gain metabolic and cardiovascular benefits by replacing the processed carbs in their diets with fat, including saturated fat, without worsening their cholesterol levels.
The new study cost $12 million and was largely funded by the Nutrition Science Initiative,a nonprofit research group. It was also supported by grants from the National Institutes of Health, the New Balance Foundation and others.
Linda Van Horn, a nutrition expert who served on the federal government’s dietary guidelines advisory committee and who was not involved with the new study, noted that the low-carb group consumed large amounts of unsaturated fat and fiber-rich vegetables — both of which are known to have beneficial effects on cholesterol and cardiovascular risk markers. The low-carb group, for example, consumed an average of 22 grams of fiber per day, which is more than the average American consumes, she said.
“While the study is valuable and carefully designed, as always innutrition research, there are many dietary factors that influence cardiometabolic risk factors that can help to explain the results,” said Dr. Van Horn, who is also chief of nutrition in the department of preventive medicine at the Northwestern University Feinberg School of Medicine.
Dr. Mozaffarian said his take home message for people is to adopt what he calls a high-fat Mediterranean style diet. It entails eating fewer highly-processed carbs and sugary foods and focusing on fruits, vegetables, nuts, seeds, fish, cheese, olive oil and fermented dairy products like yogurt and kefir. “That’s the diet that America should be focusing on. It’s where all the science is converging,” he said.
--
The physicians at Cross County Cardiology - Mt. Sinai are here to help you take care of your health. Make an appointment today by calling 201-776-8690 or go online to schedule. Your heart will thank you!
Despite increasing popularity of electronic cigarettes (e-cigarettes), the long-term health effects of habitual e-cigarette use remain unclear.1Many constituents of e-cigarette aerosols, including nicotine, carbonyl compounds, fine particulate matter, and metals, are associated with substantial toxicity.1Inhalation of e-cigarette aerosols among young, healthy adults induces inflammation and oxidative stress.1Two large cross-sectional studies reported no significant association between exclusive e-cigarette use and cardiovascular disease (CVD).2,3However, longitudinal studies are essential to assess the association of e-cigarette use with incident CVD.
Authors say fitness checks should join other, more commonly measured risk factors, given its strong prognostic value.
Cardiorespiratory fitness and age are the two most important variables for predicting all-cause mortality in patients with coronary artery disease, a new artificial intelligence (AI) study shows.